

When managing hormonal skin conditions, the choice of birth control is a critical therapeutic decision. Not all progestogens are equal. The synthetic progestins used in combined oral contraceptives carry widely varying androgenic profiles—a distinction with meaningful clinical consequences, particularly for women struggling with persistent breakouts, hair thinning, or excess facial hair.
What is a Progestogen?
Progestogens are a class of steroid hormones that bind to progesterone receptors. In the context of the combined oral contraceptive pill (COCP), a synthetic progestogen — or progestin — is paired with an oestrogen (typically ethinylestradiol) to suppress ovulation, thicken cervical mucus, and alter the endometrial environment.
All currently used progestins are classified by their structural origin. This matters because some are derived from testosterone and can inadvertently trigger skin pigmentation disorders or worsen existing acne in sensitive patients.
Generations of progestins and their androgenic character
Progestins are commonly grouped by generation, with each successive generation developed partly to reduce androgenic side effects, improve contraceptive reliability, or both.
First-generation progestins — norethisterone and ethynodiol diacetate — were developed in the 1950s and 60s. They are moderately androgenic, with androgen receptor binding affinity of approximately 15% relative to testosterone. At the high doses used in early pills, they contributed to adverse lipid profiles and androgenic side effects including acne and weight changes.
Second-generation progestins, notably levonorgestrel and norgestrel, are more potent and considerably more androgenic. Levonorgestrel has high androgen receptor binding affinity — estimated at 50–100% relative to testosterone depending on the assay system used — and is associated with the highest rates of acne and oily skin among commonly used progestins. Norgestrel is the racemic form; only the levo-isomer is biologically active, giving it approximately half the androgenic potency of equivalent-dose levonorgestrel.
Third-generation progestins — desogestrel, gestodene, norgestimate — were designed to retain progestogenic potency while minimising androgenic activity. Desogestrel and norgestimate have very low AR binding affinity (1–2% vs testosterone) and are considered low androgenic in clinical practice. Gestodene is more complex: intact-cell assays show higher AR binding than simple cytosol assays suggest, though high SHBG affinity is thought to limit free drug at tissue level, explaining lower clinical androgenicity than its receptor binding might predict.
Relative androgen receptor binding affinity of progestins
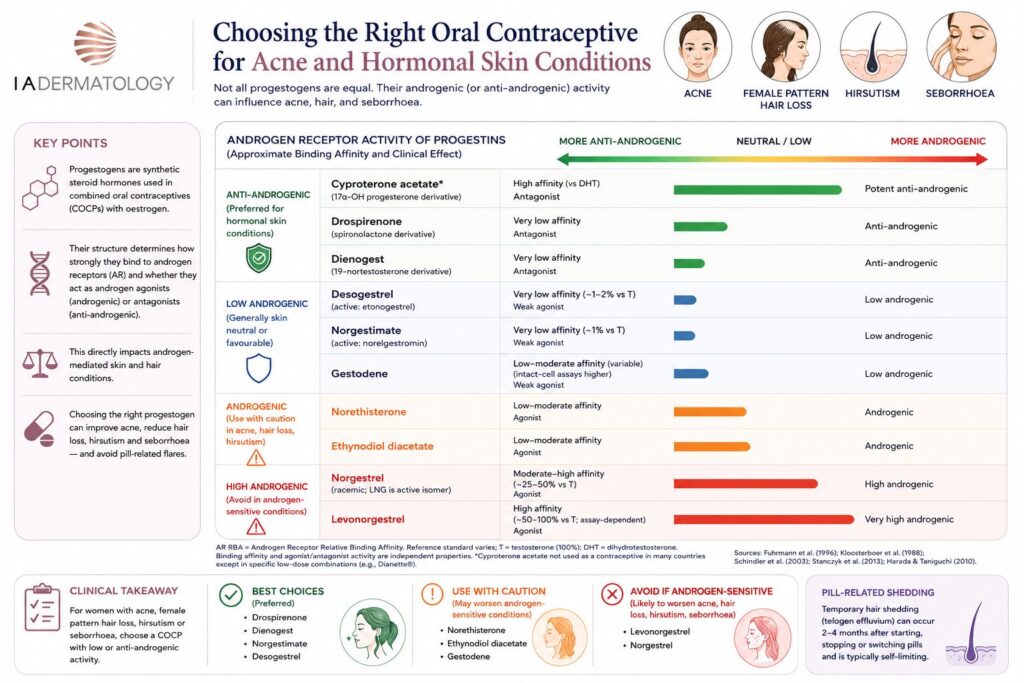
The table below summarises the androgen receptor relative binding affinity (AR RBA) of progestins used in oral contraceptives, alongside their structural classification, receptor agonism type, and clinical androgenic effect. An important distinction is made between binding affinity and functional activity — a compound can bind the AR with high affinity while acting as an antagonist rather than an agonist, as is the case with cyproterone acetate.
| Progestin | Structural origin | AR RBA (approx.) | AR agonism | Functional effect | Relative binding |
|---|---|---|---|---|---|
| 1ST GENERATION — 19-NORTESTOSTERONE DERIVATIVES | |||||
| Norethisterone | 19-Nortestosterone | ~15% vs T | Agonist | Androgenic | 🟩 🟩 |
| Ethynodiol diacetate | 19-Nortestosterone | ~15% vs T | Agonist | Androgenic | 🟩 🟩 |
| 2ND GENERATION — 19-NORTESTOSTERONE DERIVATIVES | |||||
| Levonorgestrel | 19-Nortestosterone | ~50–100% vs T assay-dependent | Agonist | Androgenic (high) | 🟩 🟩 🟩 🟩 🟩 |
| Norgestrel | 19-Nortestosterone | ~25–50% vs T racemic; LNG active | Agonist | Androgenic (high) | 🟩 🟩 🟩 🟩 |
| 3RD GENERATION — 19-NORTESTOSTERONE DERIVATIVES | |||||
| Desogestrel (active: etonogestrel) | 19-Nortestosterone | ~2% vs T | Weak agonist | Low androgenic | 🟩 |
| Gestodene | 19-Nortestosterone | ~4–30% vs T SHBG limits free drug | Weak agonist | Low androgenic | 🟩 🟩 |
| Norgestimate (active: norelgestromin) | 19-Nortestosterone | ~1% vs T | Weak agonist | Low androgenic | 🟩 |
| 4TH GENERATION — 19-NORTESTOSTERONE DERIVATIVE (ANTI-ANDROGENIC) | |||||
| Dienogest | 19-Nortestosterone | <1% vs T low binding | Antagonist | Anti-androgenic | 🟩 |
| 4TH GENERATION — SPIRONOLACTONE DERIVATIVE | |||||
| Drospirenone | Spironolactone | 0.6% vs DHT ~<2% vs T | Antagonist | Anti-androgenic | 🟩 |
| 17Α-HYDROXYPROGESTERONE DERIVATIVE — REFERENCE ANTI-ANDROGEN | |||||
| Cyproterone acetate (co-cyprindiol / Dianette) | 17α-OH Progesterone | 70–100% vs DHT high affinity | Antagonist | Potent anti-androgenic | 🟩 🟩 🟩 🟩 🟩 |
AR RBA = Androgen Receptor Relative Binding Affinity. Reference standard varies: “vs T” = vs testosterone (100%); drospirenone and cyproterone acetate values are vs DHT. Binding affinity and agonist/antagonist activity are independent properties — cyproterone acetate binds with high affinity but acts as a competitive antagonist; drospirenone and dienogest have very low binding but produce functional anti-androgenic effects in transactivation assays. Published AR binding values vary substantially according to assay system, reference ligand, receptor preparation and whether the parent compound or active metabolite is tested. The table should therefore be read as a clinical hierarchy rather than a fixed numerical ranking. Sources: Fuhrmann et al. (1996); Kloosterboer et al. (1988); Schindler et al. (2003); Stanczyk et al. (2013); Harada & Taniguchi (2010).
Why androgenic activity matters clinically
Androgens — including testosterone and its metabolite dihydrotestosterone (DHT) — act on multiple cutaneous and follicular targets. In women with underlying androgen sensitivity, the choice of progestin in the COCP can meaningfully worsen or improve four distinct clinical conditions: acne vulgaris, female pattern hair loss, hirsutism, and seborrhoea. Each condition shares the same upstream driver — excessive androgenic stimulation of target tissues — but differs in the receptor distribution and cell type involved.
Conversely, oestrogen raises sex hormone-binding globulin (SHBG), which reduces free androgen levels.
All COCPs provide this benefit to some degree. However, progestins with significant androgen receptor agonist activity can attenuate or override this benefit at the receptor level, negating the favourable oestrogen effect and perpetuating androgenic drive at target tissues.
Clinical consequences by condition
Acne vulgaris. DHT stimulates sebaceous gland hypertrophy and increases sebum production, creating the lipid-rich environment that drives Cutibacterium acnes proliferation and follicular inflammation. Progestins with androgenic activity — particularly levonorgestrel — directly worsen acne by stimulating sebaceous glands via AR agonism. Women prescribed levonorgestrel-containing pills frequently report new-onset or worsened acne, particularly on the lower face, jawline, and back. Conversely, anti-androgenic progestins reduce sebum output and improve acne lesion counts. Women with pre-existing acne who require the COCP should be counselled that progestin choice directly affects their dermatological outcome.
Female pattern hair loss (FPHL). FPHL — characterised by diffuse thinning over the crown and mid-scalp with preservation of the frontal hairline — is androgen-sensitive in a significant proportion of affected women, mediated principally by DHT acting on follicular AR to shorten the anagen (growth) phase and miniaturise follicles over successive cycles. Prescribing a strongly androgenic progestin such as levonorgestrel in a woman with FPHL can accelerate follicular miniaturisation and worsen hair loss. This is an underappreciated consequence of progestin selection: women presenting with FPHL who are on or considering the COCP should be switched to or started on a pill containing a low-androgenic or anti-androgenic progestin. Drospirenone, norgestimate, or cyproterone acetate-containing formulations are preferred. It should be noted that all COCPs can trigger a telogen effluvium on initiation or cessation, which is a separate and usually self-limiting phenomenon distinct from androgenic FPHL.
Hirsutism. Terminal hair growth in androgen-sensitive areas — upper lip, chin, sideburn distribution, chest, abdomen, and inner thighs — is driven by DHT acting on dermal papilla cells in hair follicles, converting vellus hairs to coarser terminal hairs. Androgenic progestins can maintain or worsen hirsutism by sustaining AR activation in these follicles. Anti-androgenic progestins reduce this stimulus, though hair follicle response is slow: meaningful improvement typically requires six to twelve months before a reduction in new terminal hair growth is apparent. Existing terminal hairs do not spontaneously regress and may require concurrent physical treatment. Women with polycystic ovary syndrome (PCOS) are particularly affected, and in this group an anti-androgenic COCP is strongly preferred.
Seborrhoea. Sebaceous gland activity is exquisitely sensitive to androgens; even low-level AR stimulation increases sebum secretion rate measurably. Seborrhoea — characterised by oily skin and scalp — is one of the earliest and most reliable markers of androgen excess in women. Androgenic progestins compound this by adding a direct agonist stimulus on top of any endogenous androgen excess. Anti-androgenic progestins, particularly drospirenone, produce clinically meaningful reductions in skin oiliness through sebaceous AR blockade, and this is often one of the first improvements women notice within the first one to two pill cycles.
| Clinical note: Women presenting with any combination of acne, female pattern hair loss, hirsutism, or seborrhoea who require oral contraception should be considered for a progestin with anti-androgenic activity. Prescribing levonorgestrel-containing pills in this group risks worsening all four conditions simultaneously. The progestin choice is not a minor formulary decision — it is a clinically significant therapeutic selection. |
Drospirenone: a structurally distinct progestin
Drospirenone is unique because it is derived from spironolactone rather than testosterone. It acts as a functional antagonist, meaning it blocks the androgen receptor. This makes it an excellent choice for patients also undergoing HRT treatment in London who need to balance their hormonal profile.
Its androgen receptor binding affinity is very low (0.6% vs DHT, equivalent to less than 2% vs testosterone), yet in transactivation assays it acts as a functional antagonist — binding does not activate the receptor, and it blocks androgen-stimulated transcriptional activation. This is mechanistically different from cyproterone acetate, which achieves potent anti-androgenic effect through high-affinity competitive binding (70–100% vs DHT), occupying the receptor and preventing DHT from doing so.
| Spotlight: Drospirenone’s dual mechanism 1. Androgen receptor antagonism: Despite very low AR binding affinity, drospirenone functionally blocks androgen receptor activation, opposing testosterone and DHT in sebaceous glands, hair follicles, and skin. Its anti-androgenic potency is approximately 30% that of cyproterone acetate. 2. Aldosterone receptor antagonism (anti-mineralocorticoid activity): Like spironolactone, drospirenone blocks the mineralocorticoid receptor — with affinity approximately five times that of aldosterone. This reduces sodium and water retention, producing a mild diuretic effect that can reduce premenstrual bloating, breast tenderness, and weight fluctuation associated with fluid retention. |
Drospirenone and androgen-related skin conditions
Multiple randomised controlled trials have demonstrated that drospirenone-containing COCPs significantly improve acne compared with placebo and with levonorgestrel-containing pills. The mechanism operates at two levels: increased SHBG (reducing circulating free androgens) and direct antagonism at androgen receptors in skin target tissues.
Drospirenone/ethinylestradiol (Yasmin, Yaz) has received FDA approval for treatment of moderate acne in women choosing oral contraception — one of few COCPs to carry this dual indication. In head-to-head comparison with co-cyprindiol (ethinylestradiol/cyproterone acetate 35/2 mg), drospirenone-containing pills produced comparable acne improvement at nine months, with no significant difference between the two formulations.
Dienogest: a different route to anti-androgenic activity
Dienogest, a 19-nortestosterone derivative used primarily in endometriosis treatment (Qlaira, Visanne), achieves anti-androgenic activity by a similar functional mechanism to drospirenone — very low AR binding affinity but antagonism in transactivation assays. Unlike drospirenone, it has no anti-mineralocorticoid activity and lacks the diuretic benefit. It is less commonly used in acne-focused prescribing but is relevant in women requiring treatment for both endometriosis and androgenic skin symptoms.
Safety considerations and prescribing context
Drospirenone-containing pills are generally well tolerated. The anti-mineralocorticoid activity warrants caution in women with renal impairment, adrenal insufficiency, or those taking potassium-sparing diuretics or ACE inhibitors, due to a theoretical risk of hyperkalaemia — though in healthy women at standard doses this is rarely clinically significant.
The venous thromboembolism (VTE) risk profile of drospirenone-containing pills is broadly comparable to other third-generation progestin pills, and modestly higher than levonorgestrel-containing pills — a consideration in women with additional VTE risk factors. The absolute risk remains low in healthy, non-smoking women under 35. Co-cyprindiol carries a higher VTE risk than standard COCPs and is not recommended as a first-line contraceptive; it should be reviewed once acne control is achieved.
| Clinical note: For women seeking the COCP who also have acne, female pattern hair loss, hirsutism, or seborrhoea, a preparation containing drospirenone or norgestimate is a rational first-line choice. Levonorgestrel-containing pills (Microgynon, Rigevidon) should generally be avoided in this group. Co-cyprindiol (Dianette) remains an option for severe acne where contraception is also required, but should be reviewed and switched to a standard COCP after acne control is achieved. |
Summary
The progestin component of the COCP is not pharmacologically inert with respect to androgen activity. Second-generation progestins, particularly levonorgestrel, carry high androgen receptor binding affinity and agonist activity that can exacerbate acne, female pattern hair loss, hirsutism, and seborrhoea. Third-generation progestins are low androgenic.
Drospirenone stands apart as the only spironolactone-derived contraceptive progestin, with very low AR binding (0.6% vs DHT) but functional anti-androgenic activity, plus unique anti-mineralocorticoid effects — making it the preferred progestin in women with androgen-related dermatological concerns.
An important pharmacological principle underpinning this table is that AR binding affinity and agonist/antagonist activity are independent properties: cyproterone acetate binds with high affinity but blocks the receptor, while drospirenone and dienogest bind very weakly yet still achieve functional antagonism.
References
1. Schindler AE, Campagnoli C, Druckmann R, Huber J, Pasqualini JR, Schweppe KW, Thijssen JH. Classification and pharmacology of progestins. Maturitas. 2003;46 Suppl 1:S7–S16. doi: 10.1016/j.maturitas.2003.09.014. PMID: 14670641
2. Stanczyk FZ, Hapgood JP, Winer S, Mishell DR Jr. Progestogens used in postmenopausal hormone therapy: differences in their pharmacological properties, intracellular actions, and clinical effects. Endocr Rev. 2013;34(2):171–208. doi: 10.1210/er.2012-1008. PMID: 23238854
3. Kloosterboer HJ, Vonk-Noordegraaf CA, Turpijn EW. Selectivity in progesterone and androgen receptor binding of progestagens used in oral contraceptives. Contraception. 1988;38(3):325–332. doi: 10.1016/0010-7824(88)90104-7. PMID: 3139361
4. Fuhrmann U, Krattenmacher R, Slater EP, Fritzemeier KH. The novel progestin drospirenone and its natural counterpart progesterone: biochemical profile and antiandrogenic potential. Contraception. 1996;54(4):243–251. doi: 10.1016/s0010-7824(96)00195-3. PMID: 8922878
5. Muhn P, Fuhrmann U, Fritzemeier KH, Krattenmacher R, Schillinger E. Drospirenone: a novel progestogen with antimineralocorticoid and antiandrogenic activity. Ann N Y Acad Sci. 1995;761:311–335. doi: 10.1111/j.1749-6632.1995.tb31386.x. PMID: 7625729
6. Muhn P, Krattenmacher R, Beier S, Elger W, Schillinger E. Drospirenone: a novel progestogen with antimineralocorticoid and antiandrogenic activity: pharmacological characterization in animal models. Contraception. 1995;51(2):99–110. doi: 10.1016/0010-7824(94)00015-o. PMID: 7750297
7. Louw-du Toit R, Perkins MS, Hapgood JP, Africander D. Comparing the androgenic and estrogenic properties of progestins used in contraception and hormone therapy. Biochem Biophys Res Commun. 2017;491(1):140–146. doi: 10.1016/j.bbrc.2017.07.063. PMID: 28711501
8. Harada T, Taniguchi F. Dienogest: a new therapeutic agent for the treatment of endometriosis. Womens Health (Lond). 2010;6(1):27–35. doi: 10.2217/whe.09.72. PMID: 20001868
9. Oelkers W, Foidart JM, Dombrovicz N, Welter A, Heithecker R. Effects of a new oral contraceptive containing an antimineralocorticoid progestogen, drospirenone, on the renin-aldosterone system, body weight, blood pressure, glucose tolerance, and lipid metabolism. J Clin Endocrinol Metab. 1995;80(6):1816–1821. doi: 10.1210/jcem.80.6.7775629. PMID: 7775629
10. Fuhrmann U, Slater EP, Fritzemeier KH. Characterization of the novel progestin gestodene by receptor binding studies and transactivation assays. Contraception. 1995;51(1):45–52. doi: 10.1016/0010-7824(94)00003-f. PMID: 7750284